
What the curriculum thinks you need to know:
PC_BK_58 Ultrasound: basic principles of ultrasound
PC_BK_60 Doppler effect, principle and clinical application
**This was a question in the Final FRCA Written exam twice in the last 5 years**
What you need to know (The theory):
Define Define Define…. So What is Ultrasound?
Ultrasound is sound waves at a frequency above that which is audible to humans.
The Range of human hearing is 20Hz to 20kHz, so, ultrasound is sound above 20kHz. The ultrasound machines we use are normally operating in the 1-10 MHz region.
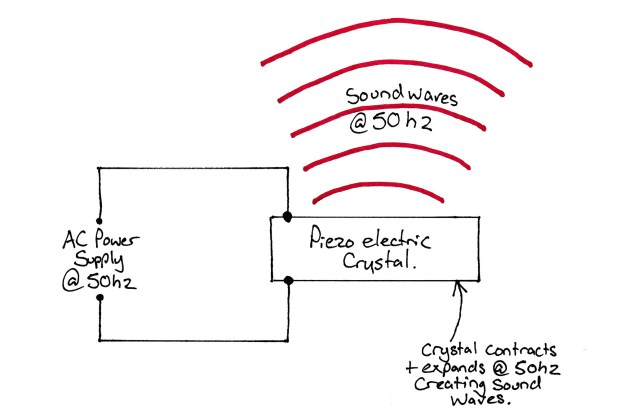
Ultrasound is generated by using piezoelectric crystals. These are crystals which have an interesting property. When they have a physical stress applied to them (ie you make them vibrate), they produce an electrical voltage.
This also works in reverse! If you apply a voltage across them then they vibrate. Interestingly, they vibrate at the frequency at the same frequency the current across them oscillates.
For example, if we put mains electricity at 50Hz through a piezoelectric crystal, it will oscillate and vibrate at 50Hz. This vibration will also produce sound waves if the amplitude if great enough.
So if we apply an alternating current with a frequency in the megahertz range then the crystal will vibrate and produce sound waves in the megahertz range. This sound can then be focussed by using acoustic ‘lenses’ and directed into a patients tissue.
The sound waves then travel through the tissue and are reflected when there is a change in tissue density or at tissue ‘interfaces’. All this means is that when one type of tissue (fat, muscle, fascia etc etc) comes into contact with another that is where the sound waves reflect.
Some of these waves (not all of them, as we’ll see later!) will be reflected back to the piezo crystals in the ultrasound transducer. These will then cause the crystals to vibrate and produce a voltage. This voltage is then interpreted by image analysis software and a ultrasound image is produced.
Image Quality
The College loves asking about the determinants of image quality.
Obviously, to make an image the ultrasound machine needs sound waves reflected back to it. So what affects the amount of sound waves reflected?
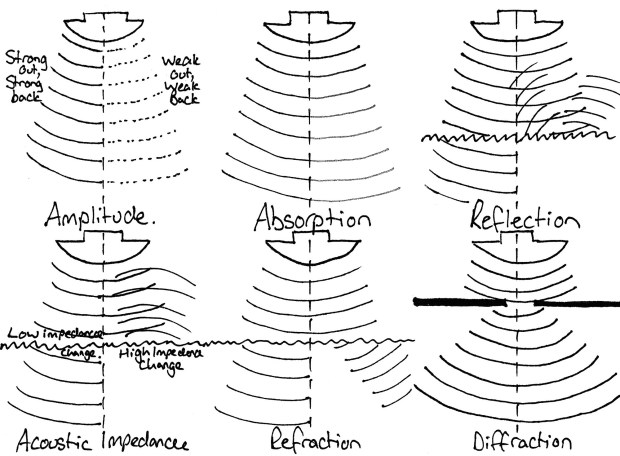
- Amplitude – The strength of ultrasound waves sent out! – The stronger the intensity of sound sent out (e.g. the better the probe) the more will be reflected. This means that more signal gets back to the probe, so it needs to be amplified less so there will be less noise.
- Absorption – The amount of the sound energy that is absorbed by the tissue. Tissue absorbs sound waves, so the amount available to be reflected back decreases.
- Reflection/Scattering – Sound waves are reflected at tissue interfaces, but not necessarily back to the probe! Smoother surfaces (think fascia) tend to reflect more reliably back to the probe, where rough surfaces scatter the sound, reflecting less back to the probe.
- Acoustic Impedance – Some molecules move less than others when subjected to vibration. This value increases with increasing density of the medium and also with increasing velocity of ultrasound wave. Higher acoustic impedance leads to decreased ability of ultrasound to travel between tissues (example: bone has very high acoustic impedance compared to soft tissue, so sound will not travel into bone reliably). If there is a large difference in acoustic impedance, then the sound wave cannot be transmitted from one to the other and is reflected backwards.
- Refraction – This is a change in beam direction at a tissue interface. This reduces the intensity of any reflected signal. It also sends sound waves in different directions below the tissue interface which can lead to image artifacts.
- Diffraction/Divergence – The spreading of an ultrasound beam with distance traveled after travelling through an obstacle. This decreases the beam intensity the deeper the beam travels as its being spread over a larger area. This is responsible for the degrading of images taken with camera with very small apertures.
All of the above is grouped together as ‘attenuation’. This just basically means that the returning beam is weaker than the beam sent out.
So These factors affect the amount of sound waves which return to the probe. But what affects the quality of the image we see?
- Amplification – If the returned signal is weak, it needs to be amplified to produce a image. Any kind of signal amplification introduces noise, which shows as a fuzzy indistinct image. This is the same reason why your IPhone pictures taken at night look noisy and not as nice as daylight photos.
- Resolution – We all know this from the higher resolution of a image, the better it looks. This is why everyone thinks that 50 megapixel camera your friend has is amazing. But in reality, resolution determines your ability to differentiate two objects. For the purposes of the exam, The higher the frequency of the ultrasound the greater the resolution. This has a byproduct, higher frequency ultrasound doesn’t penetrate tissues well, so your depth of image will be reduced if you increase your frequency.
So think about this the next time you put a central line in a morbidly obese patient… Why can’t you see the vein as clearly?
Simple, The more tissue the ultrasound has to go through, the higher the attenuation (due to all those things above…) and, you have to use a lower frequency sound wave to reach that depth hence your resolution decreases. So we have a low resolution, noisy (heavily amplified) image. Very difficult to see the vein, let alone your needle!
Doppler and The Doppler Effect
The change in apparent wavelength of a wave when the observer is moving relative to the wave source.
So, if the source or observer is moving, a wave will seem to be of a different wavelength. The easy way to think of this is an ambulance. It doesn’t change the pitch of its siren, but as it flies past you, it appears to change pitch.
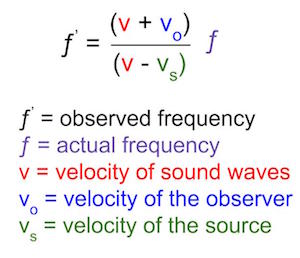
If you (the observer) stand still and the ambulance (the source of wave) moves towards you, the waves ‘squash’ together, and hence the frequency of waves appear to increase. Hence the pitch seems to get higher. The opposite occurs when the source travels away from you.
You can work out the predicted pitch with the doppler equation by knowing how fast the source is travelling:
What you need to know (How it works in practice):
There’s not much more to say about ultrasound physics with regard to clinical practice. Except they have asked about a few clinical topics related recently.
Patient factors affecting ultrasound image quality:
The college asked this in the final FRCA written exam recently. To answer this, just think of those patients which are difficult to do an ultrasound guided nerve block.
- Obesity – More subcutaneous fat means deeper structures. As we mentioned earlier, this means you need to use a lower frequency probe to get decent tissue penetration. That in turn means lower image resolution and quality.
- Oedema – Have you ever tried doing a TAP block a couple of days after abdominal surgery or an ankle block on patients with dependant oedema? Its very difficult to get views and see the different structures. If we think about what happens in oedema, everything basically gets water logged. Hence, we loose the differences between tissues in terms of density. This then makes everything look the same on an ultrasound image.
- Muscle bulk – Not so much to do with image quality per se, but cachectic patients and patients with poor tone can be more difficult to find structures. This is both due to smaller muscles (makes it more difficult to make out layers) and due to less distinct fascial planes.
Random Exam factoids (i.e. the things the college like asking):
- This topic has come up in the final FRCA written multiple times in the past 5 years. The first time it was answered very very badly (~5% pass rate!!). It was much better answered the second time, but this was likely due to the fact they published the mark scheme in the examiners report the first time (this has subsequently disappeared!)
© Sam Beckett and Physics4FRCA, 2018. Unauthorized use and/or duplication of this material without express and written permission from this site’s author and/or owner is strictly prohibited.

Thank you nice guide for trainees as well as trainers
LikeLike