
What the curriculum thinks you need to know:
PC_BK_63 Diathermy: monopolar, bipolar; safety and uses A,C,E 1
What you need to know (The theory):
The first thing you need to know: Diathermy machines make annoying noises.
The second thing you need to know: Diathermy machines muck up most of your monitoring.
The third thing you need to know: Electricity travelling through tissues causes heating. Lots of electricity travelling through tissue causes burning!
Current density
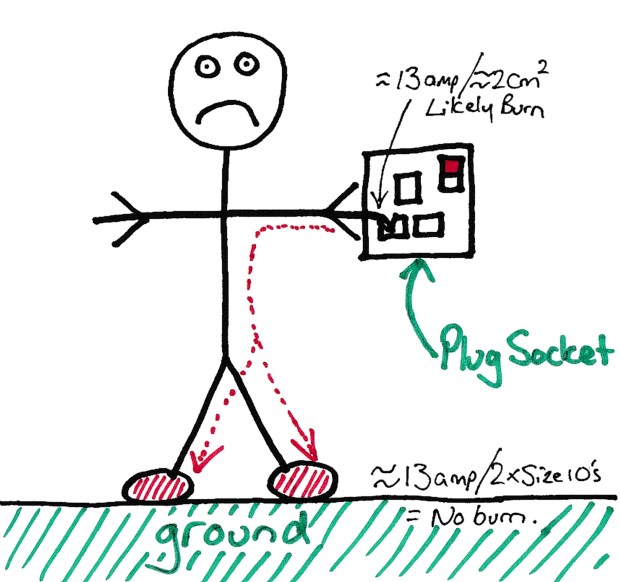
There’s numerous stories about electrocution and burnt parts of the body circulating the internet. However they all have things in common, the person involved gets burnt at a small point of contact, but their feet (which the electrical current would have to flow through to get to ground) remain relatively unscathed. Lets look at our friend Bob…
Current Density
This occurs because of the idea of current density. The current flowing through Bob’s finger is the same as that flowing through his feet. Except, that the area it flows through on his fingertip is tiny compared to that in his feet.
Current density is the current flowing divided by the area it flows through.
Current densities of less than 1 mA/mm-2 are harmless, but over about 5 mA/mm-2 cause burns.
Diathermy
Diathermy is the device we use to selectively burn (and coagulate) tissue. The premise is the same as what Bob is doing above, except from we put a large surface area pad connected to ground on him (usually on his leg) and the other point of contact is a small instrument (forceps or pen like device) which allows the surgeon to ‘aim’ the device.
The current density at the instrument end is high as the surface area is tiny, but the current density at the plate is low as it has a large surface area. Hence the tissue in contact with the instrument heats up a lot (and causes burning and coagulation) but the tissue in contact with the large surface area plate does not. (note: the leg plate DOES heat up, but just not very much. This is why the area it comes into contact with is always checked after an operation). A typical diathermy machine will produce current densities over 100 mA/mm-2 to cause heating and burning of the tissue.
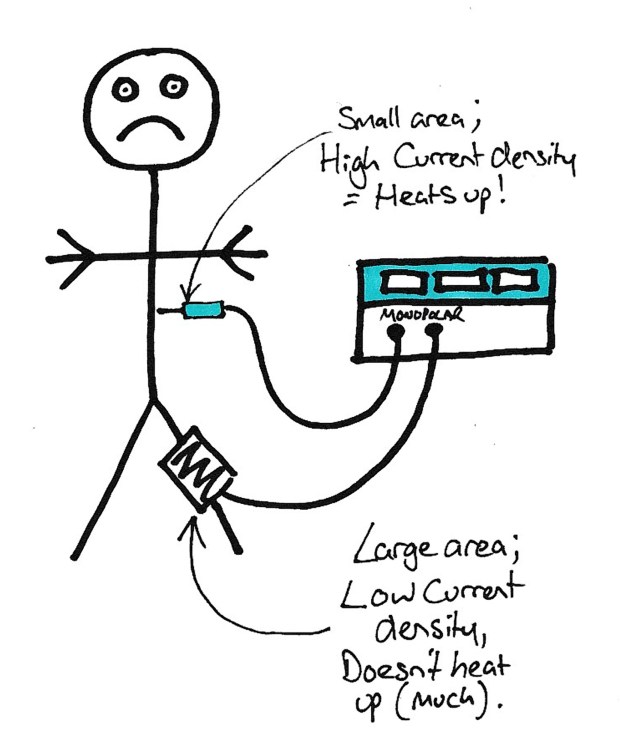
Basic Monopolar Diathermy Setup
Now, the other thing that happened to Bob at the top of the page is he had a slight heart problem. Electrical current tends to interfere with nerve and heart function (hence the stories of not being able to let go of electrical sources and them causing people’s hearts to stop). So how do we get around that?
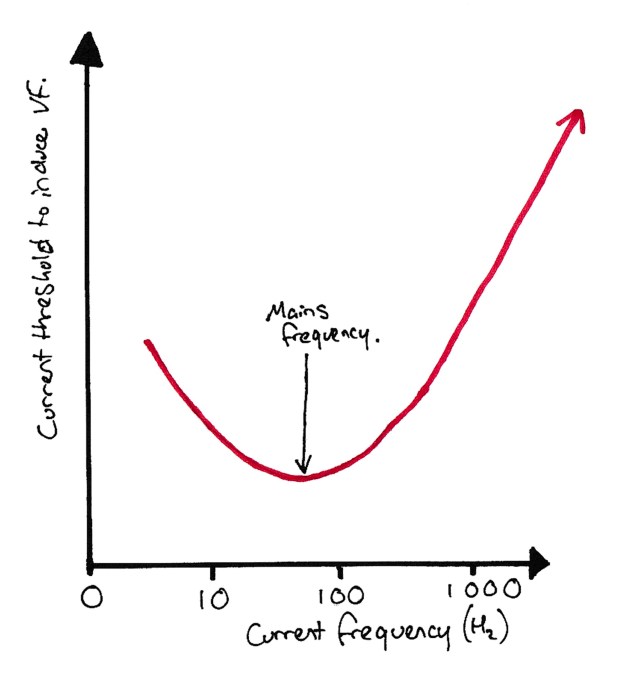
VF Potential against Current Frequency… Mains Frequency is BAD.
Electricity has different potential to cause ventricular fibrillation depending on its frequency. The peak potential to cause VF occurs at ~50hz. This is a bit problematic as that is mains frequency. Note this isn’t chosen as mains frequency to cause as many cases of VF as possible, its because its the frequency which ‘won’ during the standardisation of electricity supply (supply used to have loads of different frequencies).
So to reduce the fibrillation potential, diathermy machines typically use very high frequencies (0.5-3.0MHz is typical).
Bipolar diathermy is another type of diathermy. This typically uses a pair of forceps with an electrode on each of the prongs. This removes the need for the leg plate. The downside of this type of diathermy is it tends to be less powerful and hence less effective.
There are different patterns of current (e.g. continuous vs pulsed) which have different effects. You’ll often hear the surgeons asking to ‘increase the coag’ or similar. This is referring to the two main modes – Cut (usually yellow) and Coag (usually blue).
If you’ve ever noticed the two pedals or buttons on the diathermy handle, this is what they’re for. Each gives a different waveform:
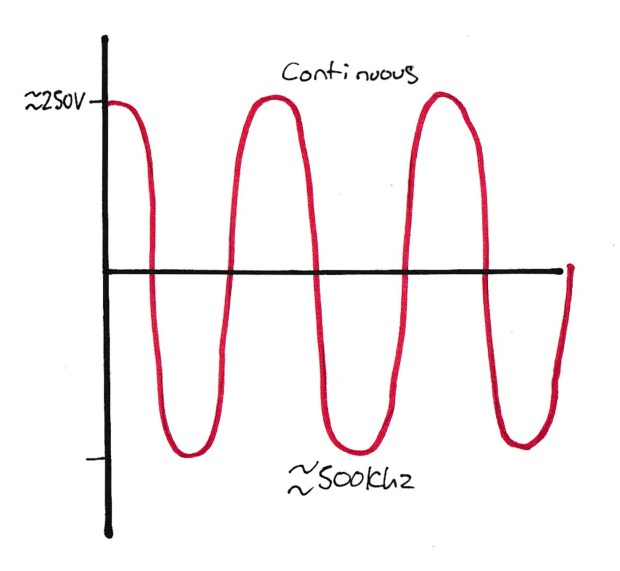
Example of a cutting diathermy waveform
Cutting uses a continuous waveform with a fairly low voltage. This gives a nice clean cut but isn’t particularly good for haemostasis. You’ll see some surgeons use this mode to open the skin at the start of an operation rather than using a scalpel.
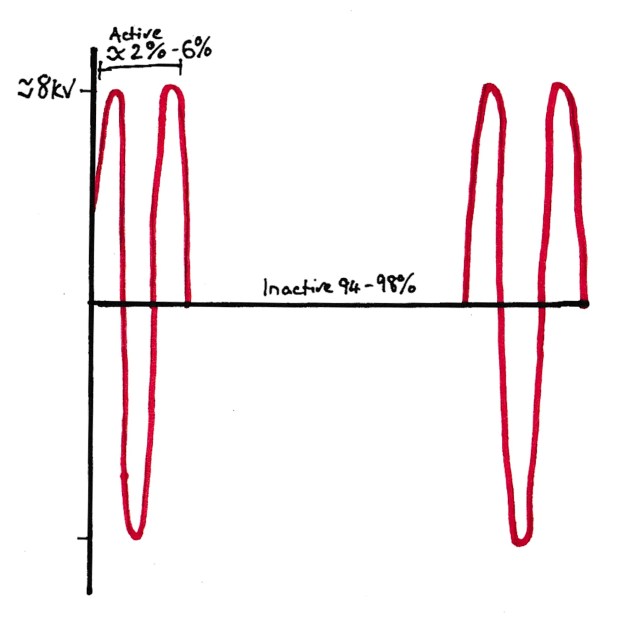
Coagulation Waveform example. Note how the current is pulsed and inactive most of the time with a very high voltage applied.
Coagulation uses pulsed waveforms with a high voltage. Typically whilst the cutting mode is continuous, coagulation modes are only active <10% of the time. You’ll see this used to seal bleeding vessels and notice it doesn’t cut very well!

Example of a blended waveform. Note the ‘in between’ values. Current present about half the time and intermediate voltage.
But, what if we want to cut and stop the cut bleeding? Well mix it up a bit. 50:50 on and off time, moderate voltage and voila…. A Blended mode that cuts and coagulates (some surgeons would argue that yes it does both, but does neither THAT well!).
What you need to know (How it works in practice):
Sources of diathermy burns:
Part of patient touching a grounded object (e.g. metal on the operating table) – This usually needs a faulty connection to the patient leg plate as the leg plate usually has less resistance to earth so current will preferentially flow that way.
Leg plate coming off the patient – If the leg plate comes partially off the patient then the surface area of contact decreases and the current density increases. This leads to increased tissue warming around the leg plate and the potential of burns. Note with modern machines, they monitor the impedance through the plate. This will increase if it is peeling off and the machine will alarm and stop working.
Diathermy and Implantable Devices:
Implantable devices such as pacemakers and spinal cord stimulators are at risk of damage from the electrical current in diathermy usage. The sites where the leads from the pacemaker insert are most at risk. The high current density at these sites leads to heating and burns. This can lead to failure of the device to stimulate the heart (and hence failure of the pacemaker) or an increase in impedance of the tissues meaning the pacemaker needs more energy to stimulate the heart, which can in turn lead to an increase in drain of the battery.
Internal defibrillators are even worse, they can misinterpret the diathermy as VF and shock the patient! Not good if the patient is awake! These devices should be deactivated prior to surgery to ensure this doesn’t happen.
The general recommendation is to try and limit the diathermy usage to bipolar in patients with implantable devices for this reason.
A note on monitoring…. You’ve probably all seen ECGs go weird when diathermy is used. But bear in mind that all monitors of electrical function or monitors that use electricity will do the same. So if you look at a BIS monitor when diathermy is used you’ll notice that the SQI (measure of the quality and hence reliability of the monitor) drop like a brick, making the monitor unreliable. The same thing happens with an oesophogeal Doppler probe. The electricity from the diathermy causes vibrations in the piezo crystals making them go a bit wacky.
Free tip: turn the volume on the Doppler probe up when the surgeons are using the diathermy….
Random Exam factoids (i.e. the things the college like asking):
- There is a theoretical risk of smoke and contaminant inhalation when using diathermy. Although this is unlikely to carry any infective tissue due to burning of the tissue, there is a worry about carcinogenic effects in the smoke. Some units use smoke removal devices to reduce this risk.
© Sam Beckett and Physics4FRCA, 2018. Unauthorized use and/or duplication of this material without express and written permission from this site’s author and/or owner is strictly prohibited.
